
Fixation After Lumbar Decompression: Is Soft Stabilization an Effective Option?
- sukanyarao
- Mar 25
- 3 min read

Lumbar spinal stenosis is a common cause of back and leg pain in older adults. When conservative treatment fails, surgical decompression is performed to relieve neural compression and improve function.
While decompression restores space for neural structures, maintaining segmental support remains an important consideration. This raises an important clinical question; how can stability be maintained without increasing surgical disruption?
Traditional Approaches to Stabilization
Spinal stability following decompression is often achieved using pedicle screw–rod constructs, which provide rigid fixation by anchoring screws into the vertebral pedicles and connecting them with rods.
Although effective, these constructs require greater surgical exposure and may contribute to adjacent segment degeneration. As a result, there has been increasing interest in less disruptive methods of stabilization in appropriately selected patients.
Soft Stabilization Through Posterior Fixation
One such approach involves soft stabilization through the posterior elements of the spine, particularly the spinous processes.
Interspinous fixation devices are placed between adjacent spinous processes to provide posterior fixation. By maintaining distraction between vertebrae, these implants help support the segment while also contributing to indirect decompression by increasing foraminal space.
In addition to the direct decompression performed surgically, this indirect effect may further relieve neural compression. Devices such as the Inspan™ interspinous fixation system are designed to provide this combination of posterior fixation and soft stabilization without the use of pedicle screws or interbody cages.
Evidence From a Prospective Clinical Study
A prospective clinical study published in the Journal of Spine Surgery in 2023 aimed to evaluate the outcomes of interspinous fixation used as a stand-alone treatment for lumbar spinal stenosis at the L4–L5 and L5–S1 levels, with comparison to historical open laminectomy data.
A total of 100 patients underwent midline decompression followed by interspinous fixation and were followed for five years. Patients were treated at the L4–L5 (n = 55) and L5–S1 (n = 45) levels.
At L5–S1, VAS improved from 8.6 to 2.2 and ODI from 39.3 to 14.7. At L4–L5, VAS improved from 8.9 to 1.7 and ODI from 41.9 to 14.2. Procedures were completed in less than one hour with low blood loss. No implant-related complications were reported, and revision rates remained low at 4.4% (L5–S1) and 1.8% (L4–L5) over five years.
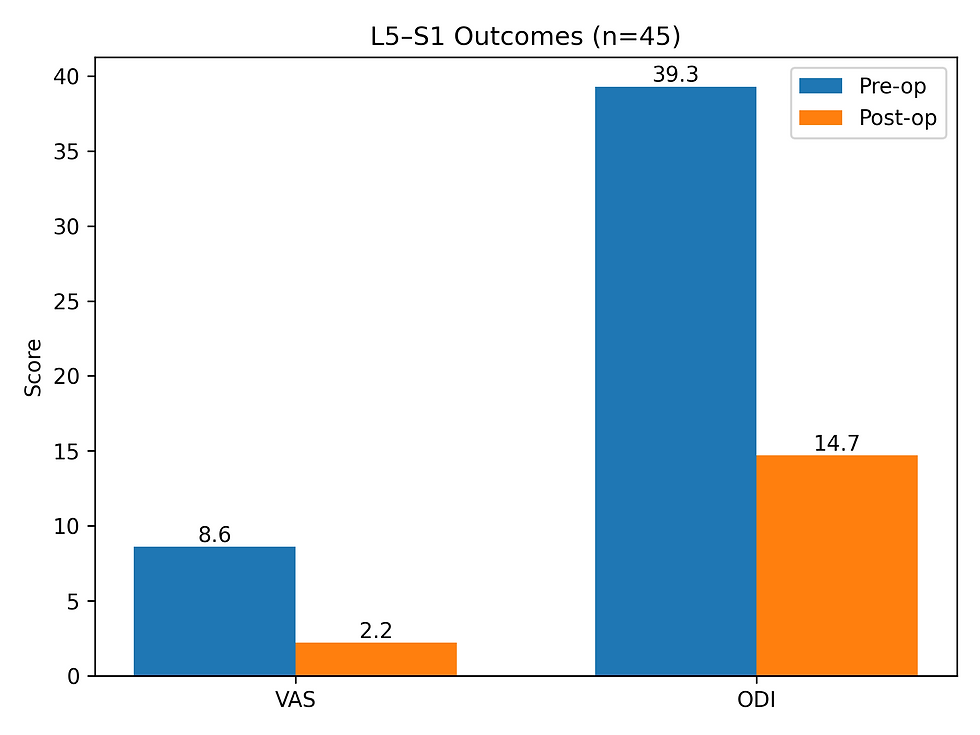
Image 1: Bar chart showing improvement in pain (VAS) and disability (ODI) following decompression with interspinous fixation at the L5–S1 level (n = 45).

Image 2: Bar chart showing improvement in pain (VAS) and disability (ODI) following decompression with interspinous fixation at the L4–L5 level (n = 55).

Image 3: Postoperative radiographs (lateral and anteroposterior views) demonstrating interspinous fixation at the L5–S1 level.
Image Source: https://pmc.ncbi.nlm.nih.gov/articles/PMC10772657/ Clinical Perspective
Findings from this study demonstrate that patients treated with midline decompression and interspinous fixation used as a stand-alone device at the L4–L5 and L5–S1 levels showed improved clinical outcomes, with low complication and revision rates over five years. Outcomes were comparable to historical laminectomy data, suggesting this approach may serve as an alternative in selected patients.
Appropriate implant sizing to achieve adequate distraction may be an important consideration to optimize neural decompression and reduce the risk of recurrent symptoms
Key Takeaway
Decompression combined with interspinous fixation demonstrated sustained improvements in pain and function over five years without the use of pedicle screws and rods.
The ability to treat the L5–S1 level, a segment often considered challenging for interspinous devices, highlights its utility in appropriately selected patients who may not be a candidate for traditional lumbar fusion.
Interested in exploring the full study and clinical data?
Read the original publication on PubMed: https://pubmed.ncbi.nlm.nih.gov/38196724/


Comments